occurred in 14 (88%) patients; the most common being neutropenia (44%; n=7), pneumonia (31%;
n=5), lymphopenia (25%; n=4), and thrombocytopenia (25%; n=4). One patient had TEAEs leading to
treatment discontinuation. No grade 5 TEAEs occurred. Infusion-related reactions occurred in 4 (25%)
patients (all grade 1/2), mainly during the first cycle.
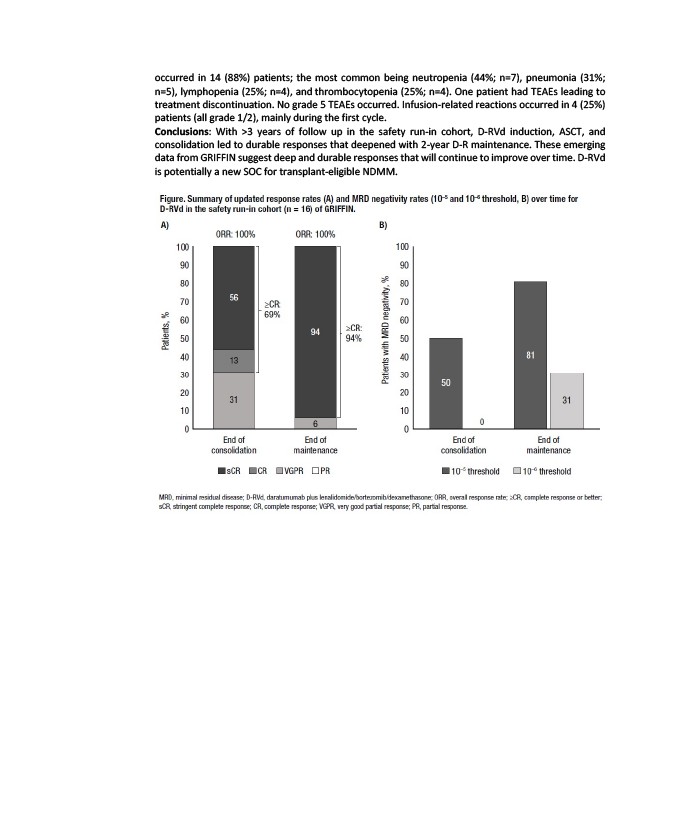
Conclusions: With >3 years of follow up in the safety run-in cohort, D-RVd induction, ASCT, and
consolidation led to durable responses that deepened with 2-year D-R maintenance. These emerging
data from GRIFFIN suggest deep and durable responses that will continue to improve over time. D-RVd
is potentially a new SOC for transplant-eligible NDMM.