SCIENTIFIC PROGRAMME
SESSION I
HOW I TREAT
SMOLDERING MYELOMA
(SMM)
SESSION II
HOW I TREAT NEWLY
DIAGNOSED MULTIPLE
MYELOMA
SESSION III
FROM RISK
STRATIFICATION TO
RISK-BASED THERAPY?
DEBATE 1
SHOULD WE USE MRD
TESTING TO DETERMINE
THERAPY IN MULTIPLE
MYELOMA?
DEBATE 2
IS THERE A FUTURE ROLE
OF AUTOLOGOUS STEM
CELL TRANSPLANTATION?
SESSION IV
HOW I TREAT RELAPSED
MULTIPLE MYELOMA
DEBATE 3
SHOULD EVERY PATIENT
RECEIVE DARATUMUMAB
IN FIRST LINE?
ROUNDTABLE
MULTIPLE MYELOMA
FROM THE PERSPECTIVE
OF FDA/EMEA AND
FOUNDATIONS
SESSION V
YOU CAN’T BE IMMUNE
FOR IMMUNE THERAPY
ANYMORE
SESSION VI
OTHER PLASMA CELL
DYSCRASIAS
KEYNOTE LECTURES
THE FUTURE OF
MULTIPLE MYELOMA
SELECTED ABSTRACTS
FOR AN ORAL
PRESENTATION
ABSTRACTS SELECTED
AS POSTERS
DISCLOSURES POSTER 4
FLOWER-LIKE PLASMA CELL NUCLEI IN MULTIPLE MYELOMA
Abibatou Sall, Moussa Seck, Seynabou Fall, Blaise Félix Faye, Macoura Gadji, Fatou Samba Ndiaye,
Saliou Diop and Awa Oumar Touré
Hematology, Cheikh Anta Diop University, Dakar, Senegal
A 43-year-old Senegalese man with no known past medical history was referred to our hospital for
asthenia and bone pain.
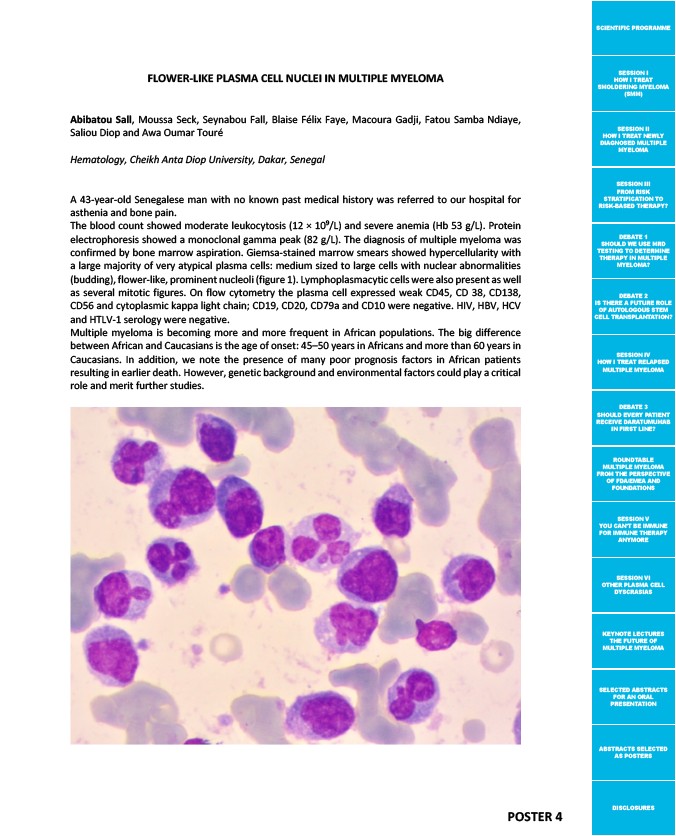
The blood count showed moderate leukocytosis (12 × 109/L) and severe anemia (Hb 53 g/L). Protein
electrophoresis showed a monoclonal gamma peak (82 g/L). The diagnosis of multiple myeloma was
confirmed by bone marrow aspiration. Giemsa-stained marrow smears showed hypercellularity with
a large majority of very atypical plasma cells: medium sized to large cells with nuclear abnormalities
(budding), flower-like, prominent nucleoli (figure 1). Lymphoplasmacytic cells were also present as well
as several mitotic figures. On flow cytometry the plasma cell expressed weak CD45, CD 38, CD138,
CD56 and cytoplasmic kappa light chain; CD19, CD20, CD79a and CD10 were negative. HIV, HBV, HCV
and HTLV-1 serology were negative.
Multiple myeloma is becoming more and more frequent in African populations. The big difference
between African and Caucasians is the age of onset: 45–50 years in Africans and more than 60 years in
Caucasians. In addition, we note the presence of many poor prognosis factors in African patients
resulting in earlier death. However, genetic background and environmental factors could play a critical
role and merit further studies.