the study in both groups. Serious treatment-related AEs were stomatitis, herpes zoster
infection, varicella zoster infection, and disseminated tuberculosis (each n=1). No colitis/dose-limiting
diarrhea/rash occurred. In QD/QW and QD, 18/33 and 10/20 patients interrupted
parsaclisib, and 4/33 and 4/20 interrupted ruxolitinib for AEs.
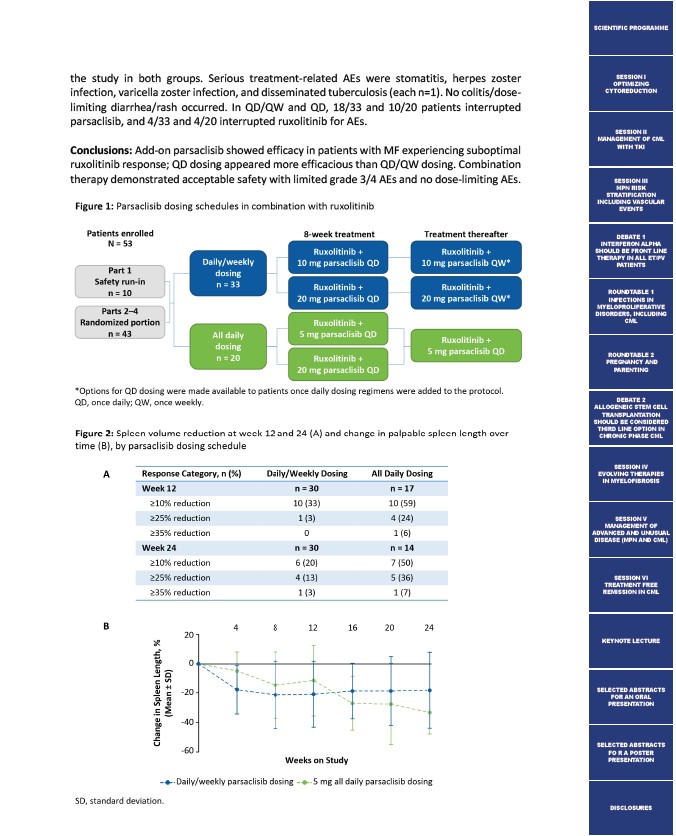
Conclusions: Add-on parsaclisib showed efficacy in patients with MF experiencing suboptimal
ruxolitinib response; QD dosing appeared more efficacious than QD/QW dosing. Combination
therapy demonstrated acceptable safety with limited grade 3/4 AEs and no dose-limiting AEs.
SCIENTIFIC PROGRAMME
SESSION I
OPTIMIZING
CYTOREDUCTION
SESSION II
MANAGEMENT OF CML
WITH TKI
SESSION III
MPN RISK
STRATIFICATION
INCLUDING VASCULAR
EVENTS
DEBATE 1
INTERFERON ALPHA
SHOULD BE FRONT LINE
THERAPY IN ALL ET/PV
PATIENTS
ROUNDTABLE 1
INFECTIONS IN
MYELOPROLIFERATIVE
DISORDERS, INCLUDING
CML
ROUNDTABLE 2
PREGNANCY AND
PARENTING
DEBATE 2
ALLOGENEIC STEM CELL
TRANSPLANTATION
SHOULD BE CONSIDERED
THIRD LINE OPTION IN
CHRONIC PHASE CML
SESSION IV
EVOLVING THERAPIES
IN MYELOFIBROSIS
SESSION V
MANAGEMENT OF
ADVANCED AND UNUSUAL
DISEASE (MPN AND CML)
SESSION VI
TREATMENT FREE
REMISSION IN CML
KEYNOTE LECTURE
SELECTED ABSTRACTS
FOR AN ORAL
PRESENTATION
SELECTED ABSTRACTS
FO R A POSTER
PRESENTATION
DISCLOSURES